These are the illustrations created live during our workshop today by Camille Aubry: they really capture the essence of a very productive morning. You can read more about today’s workshop on Twitter (search for #IllnessAsFiction).

Illness as Fiction: Textual Afflictions in Print and Online
A research project on factitious illness narratives
These are the illustrations created live during our workshop today by Camille Aubry: they really capture the essence of a very productive morning. You can read more about today’s workshop on Twitter (search for #IllnessAsFiction).

I’m delighted to announce that registration is now open for the workshop “Autofiction and Illness Narratives”, an exciting coda to this project!
The workshop will take place online on Wednesday 9th June 2021 10am-12pm BST. We will be joined by Graham Matthews (Nanyang Technological University, Singapore), Olga Michael (University of Cyprus), and Abby Ashley (University of Bristol) to learn more about their work at the intersection of autofiction, illness narratives scholarship, graphic medicine, and critical disability studies. The presentations will be followed by a discussion on how theories of autofiction can help us make sense of fake illness narratives and life-writing, more in general.
Attendance is free, but please email maria.vaccarella@bristol.ac.uk to book your place.
The third and final workshop for the Illness as Fiction project was held at the University of Bristol on the 25th January 2019. Led by Dr Maria Vaccarella, the session consolidated many of the ideas explored in the previous workshops, and focused on Factitious Disorder, Fabricated or Induced Illness, and factitious HIV/AIDS narratives. My research considers the limitations of linear and triumphalist illness narrative conventions when expressing female autistic experience. As a regular participant in Maria’s workshops, I have been particularly interested in how factitious illness narratives appear to employ such conventions as a means to appeal to the reader’s empathetic faculties.
On this note, the ice-breaker exercise invited us to email Maria with a fake illness story, and explain why we were ‘missing’ the workshop.
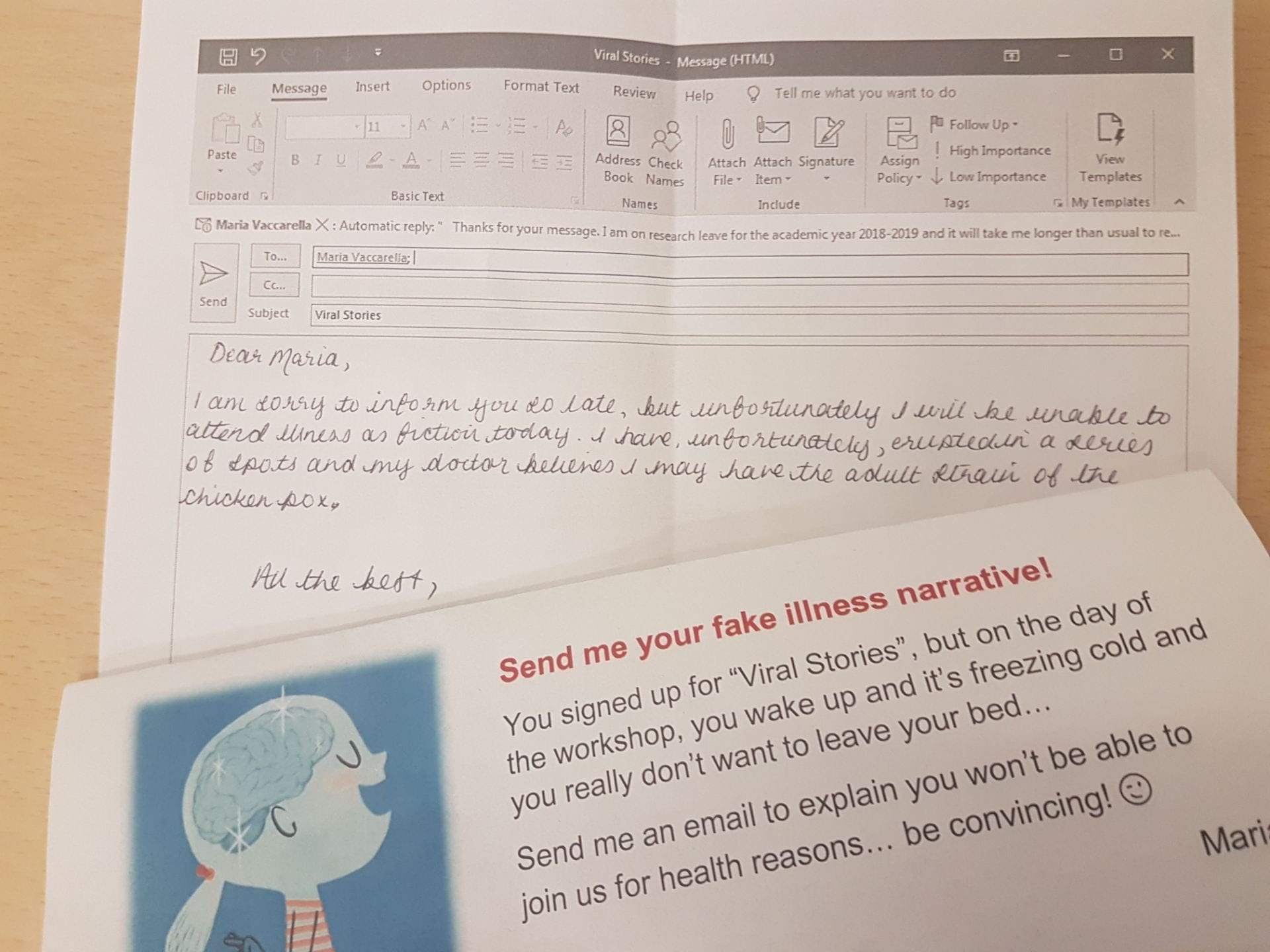
Although it is unlikely that my effort was in any way believable, the task made me think a lot about how we talk about illness, and what kinds of literary devices may be used by those who do fabricate illness.
Maria began with an overview of the previous workshops and a project update, which included mention of Louise Benson James’s recent interview with Professor Lisa Bortolotti about the ERC-funded PERFECT project, and Maria’s upcoming presentation on Illness as Fiction at King’s College, London on the 27th February. She also provided us with an update on James Frey whose factitious memoir, A Million Little Pieces, was discussed in earlier workshops. Although his 2018 novel, Katerina, has garnered significant media coverage, Sian Cain of The Guardian has argued that, despite gaining fame through deception, writers like Frey continue to flourish by capitalising on such attention.
The morning session involved two presentations relating to factitious narratives of illness. The first talk was from Dr Christopher Bass, Consultant in Liaison Psychiatry in Oxford and expert in Factitious Disorder (Munchausen syndrome) and Fabricated or Induced Illness (FII, or Munchausen’s-by-proxy). Christopher discussed his experience of working with over 50 cases of FII, the condition in which an individual deliberately imposes illness upon another person, usually a child, and results in significant and lasting harm to the victim. He also referred to several high-profile cases, including the nurse Beverley Allitt who attacked 13 children (4 of whom were killed) for attention. By studying Allitt’s entire medical history, it was clear that her own Factitious Disorder had been transferred to her victims during the period of abuse. Although the perpetrator’s motives are unknowable and are inevitably complex, Christopher explained that the care-eliciting behaviour which characterises FII likely results from feelings of emptiness, and a need for care and attention.
Next, we heard from Dr Anita Lavorgna, who lectures in Criminology at the University of Southampton, and has written extensively on cybercrime and organised crime. Anita is investigating the potential harm of Complementary and Alternative Medicine (CAM), which are approaches to illness developed outside of western medicine. Although proponents of CAM are not necessarily committing a crime, they partake in the act of ‘respectable deviancy’ because treatments are often untested, informed by pseudoscience, and are far more likely to harm than benefit the patient. Anita discussed the respectable deviancy of Belle Gibson, whose fabricated claim of cancer, and its management through diet and alternative medicine was investigated in Maria’s first workshop. Interestingly, as Gibson’s deviancy was exposed by online debunkers and eventually reached mainstream media, her narrative changed. Her constructed image of a mother, survivor, and businesswoman was replaced with a narrative of justification, and then of trauma, victimhood and a lack of responsibility. Anita also reflected on the problem of intervening in factitious narratives such as Gibson’s, due to the individual’s right to speak freely.
The talks incited vigorous and thought-provoking questions and discussion. Particular interest lay in the higher prevalence of women with FII, the slippery borderline between illness anxiety and deception, and the mental health issues which often accompany FII. We also considered respectable deviancy in relation to the ‘anti-vax’ movement, and how media articles relating to CAM often, problematically, present doctor and celebrity opinions with equal credibility. With so many fascinating strands of enquiry, it was unsurprising that we ended up running into the break!
The afternoon consisted of collaborative activity and roundtable discussions. Returning to Susan Sontag’s claim that cancer and HIV/AIDS are especially prone to metaphorical distortion, Maria explained how HIV/AIDS has been perceived in terms of contagion and subversion, ‘something total, civilisation threatening’ (Sontag, 1989, p. 149). We were presented with a series of passages from HIV/AIDS literature to explore the boundaries between memoir and the novel. With autofiction also entering the mix, it was a challenging task! It did, however, provide valuable insight into how particular approaches to narrating illness influence both literary forms. Maria explained how these narratives have changed in light of medical advancements, and that it can be difficult to reconcile the graphic descriptions from the 1980s with today’s experience, where a person living with HIV may appear physically fit, but often hides the trauma of having witnessed many deaths in their community. She was also keen to remind us that, although we concentrate on singular examples, the history of AIDS is also the unprecedented history of communities coming together.
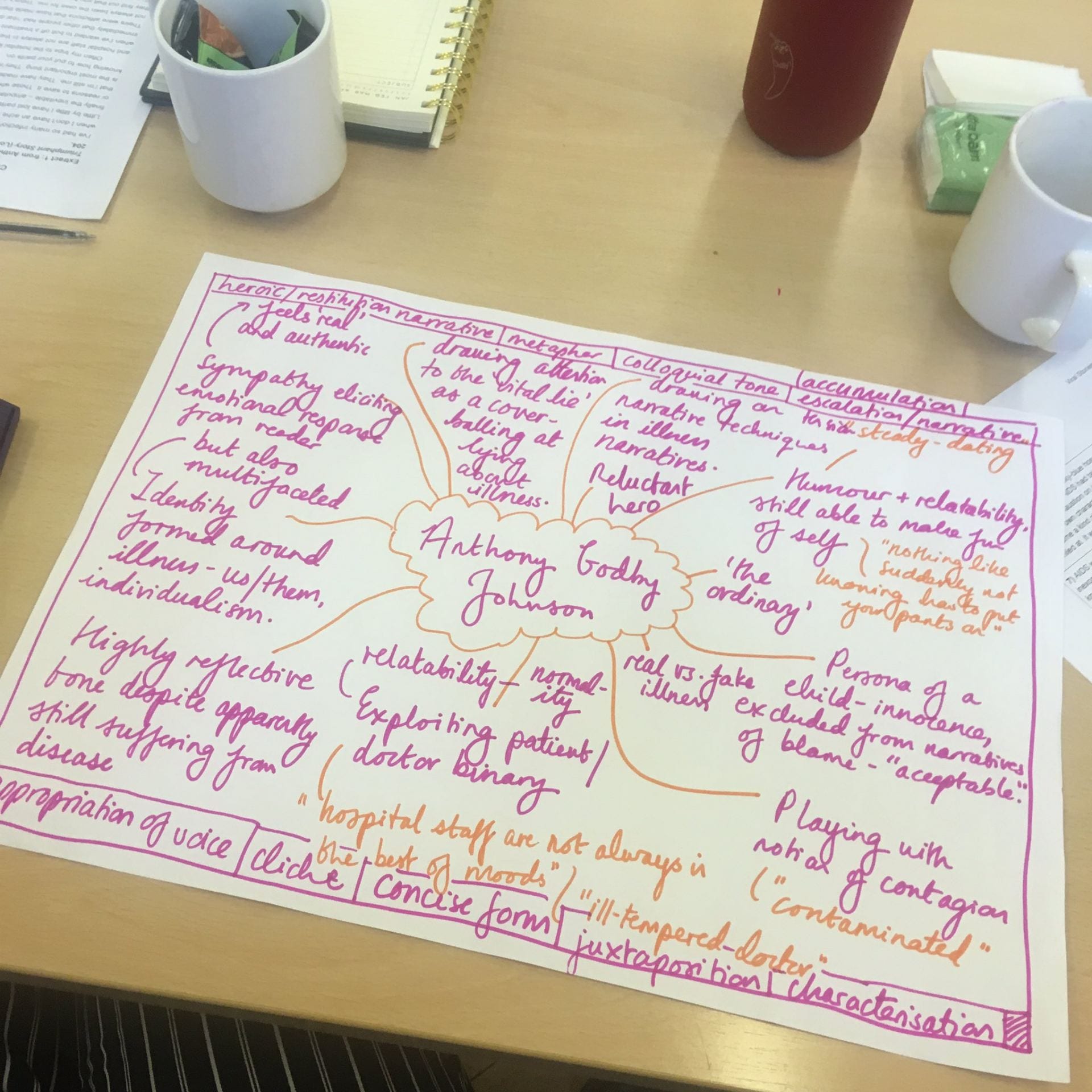
It was with a natural progression, then, that we discussed HIV/AIDS in the context of a literary community. We learned about Anthony Godby Johnson’s narrative, A Rock and a Hard Place: One Boy’s Triumphant Story (1993), which attracted attention and support from prominent HIV/AIDS activists. However, not only was the story revealed to be completely fabricated, it was also apparent that Anthony was a fictional creation of Joanne Vicki Fraginals who claimed to be his adoptive mother, ‘Vicki Johnson’. Consequently, Johnson’s narrative reveals a curious instance of virtual Munchausen’s-by-proxy. Maria’s engagement with Anne Rothe’s interpretation of Johnson’s case was particularly interesting. In Popular Trauma Culture: Selling the Pain of Others in Mass Media, Rothe suggests that, with the interest of real-life writers in ‘Anthony’ and his later emergence as an online persona by a second perpetrator, this instance of FII has become a kind of literary work in itself (2011, p. 128).
Our final task was to consider the memoir and Armistead Maulpin’s rewriting of Fraginals’s deception, The Night Listener (2000). We located literary devices which facilitate an emotional experience that offers, in the words of Alyson Milner, ‘a different kind of real’ (2012, p. 96). This led to discussions about how the writers attempt to elicit empathetic responses through notions of innocence, doctor/patient relationships, stigma, and the representation of the self as ‘normal’ despite being ill.
It was with a thought-provoking end to the workshop, then, that discussion turned to consider the expression of illness more widely. It brought into sharp relief the ways in which we communicate illness to medical professionals, our peers and in literature, and how notions of judgement or disbelief may influence such expression.
I’m delighted to announce that registration is now open for our third and final workshop “Viral Stories”.
For the morning session, we will be joined by two guest speakers: Christopher Bass (Oxford), who will present his work on factitious disorder, and Anita Lavorgna (Southampton), who has worked on Belle Gibson in the context of deviant behaviour. The collaborative textual analysis session in the afternoon will be devoted to HIV/AIDS narratives this time.
Join us if you are interested in factitious illness memoirs, autofiction or, more in general, in the overlap between psychiatry, criminology, and literature!
Attendance is free and lunch will be provided, but places are limited, so please book here.
Looking forward to seeing you in Bristol on 25th January!
In this post we interview Professor Lisa Bortolotti about her ERC-funded project Pragmatic and Epistemic Role of Factually Erroneous Cognitions and Thoughts (PERFECT). Project PERFECT aims to establish whether cognitions that are inaccurate in some important respect can ever be good from a pragmatic or an epistemic point of view.
Lisa is a philosopher based at the University of Birmingham who works on ‘the limitations of human cognition and human agency, investigating faulty reasoning and irrational beliefs, delusions, confabulations, distorted memories, poor knowledge of the self, unreliable self narratives, self-deception, inconsistencies between attitudes and behaviour, unrealistic optimism, and other positive illusions’. Lisa has edited and contributed to a book that has been just published open access; Delusions in Context (Palgrave 2018). It is an exploration of delusions—unusual beliefs that can significantly disrupt people’s lives. It includes contributions from experts in clinical practice, psychology, cognitive neuroscience, and philosophy.

How did you first start thinking about the idea that delusions might perform a beneficial role?
In my post-doctoral research I became increasingly committed to defending one version of the continuity thesis. This is the idea that the irrationality of the unusual beliefs people report in the context of schizophrenia, dementia and other mental health issues (so called clinical delusions) is not qualitatively different from the irrationality of more common superstitious or prejudiced beliefs. In both cases, we tend to adopt beliefs that are not well supported by evidence and are not responsive to counterevidence. Superstitious and prejudiced beliefs are just more widely shared.
One thought that people often have about everyday irrational beliefs is that they fail epistemically (that is, in their relationship with evidence), but have other advantages that may begin to explain why we hold onto them so tenaciously. So, it may be false that wearing my lucky suit will bring me luck in the job interview, but it is a fact that when I wear that suit I feel more confident and less nervous. I began to ask whether the same was true of delusional beliefs. Could it be that there is some benefit in adopting or maintaining them? Could this benefit explain why giving up a delusional belief is so hard, and often leads to severe depression and suicidal thoughts? I was genuinely curious about such questions and did not know whether there was any literature on this. It turns out that there was very little out there—some clinicians had written about “successful psychotics” or about the “adaptive nature” of delusion formation.
So, I started from there. My view now is that in some cases the adoption of a delusional belief offers temporary relief from anxiety and, depending on the content of the belief itself, may have some protective function, that is, it helps the person avoid negative thoughts or emotions about herself. If your readers want to know more, they can check four open access papers: on delusions in schizophrenia, on delusions in depression, on delusions as protective, and on motivated delusions.
Can you give us an everyday example in which beliefs which include an irrational or delusional element have had a benefit of some sort – either to you personally or to people generally?
Yes, of course. In her influential book on positive illusions, Shelley Taylor argued that we all tend to adopt beliefs about ourselves that are optimistically biased, unless we experience depressive symptoms. So, a mentally healthy person is likely to believe that she is better than average in some domains (attractiveness, intelligence, kindness, etc.) even if the evidence at her disposal suggests that this is not the case. In a study conducted in the States in the Seventies, for instance, academics were asked whether they thought they were doing better research than average in their field, and 94% of them replied that they thought they did. Not all of them can have been right about that!
So, we do have an overly optimistic view of our talents and skills (this bias is called the superiority effect or the better-than-average effect). This means that we have epistemically irrational beliefs. We have beliefs about ourselves that are not well supported by evidence: we tend to remember our successes but forget our failures, which obviously skews our evidence about our competence in some domain. Our beliefs are not responsive to evidence either: when we get new evidence of our failures we tend not to update our beliefs accordingly, but we are very happy to update them when we get evidence of our successes. Are such biased beliefs beneficial?
Well, I think they are. Taylor argued that positive illusions are necessary for mental health. They enhance our wellbeing and increase our productivity. I was struck by the role that these positive illusions can play in supporting our agency: we are more likely to preserve our motivation to pursue our goals in the face of obstacles, and to attain our goals as a result of this perseverance, when we believe that we are skilled and successful. I defend this view in a paper on optimism, success, and agency (open access).
Your project is concerned with stories: ones that we tell ourselves and others, constructing self-narratives which can often support personal agency. Can you tell us a bit about whether your project crosses over with literary studies at all? It reminded me of folk tales and fairy tales, stories with confabulated elements but a social safe-keeping function, e.g. warning children away from doing something dangerous.
This is a very interesting question. For project PERFECT we have collaborated with psychologists and psychiatrists, mental health activists and people with lived experience of mental health issues, but we haven’t interacted much with researchers in the medical humanities, social science, or linguistics and literature. This is probably because we were having a focus on the connection between rationality and mental health, and because at the time of planning our activities I hadn’t realised how crucial the notions of self-image, self-concept, and self-narrative would have become for our investigation.
For my next project, I have filled the obvious disciplinary gap and involved from the start both linguists who are interested in shared meanings and self-image (on traditional media and social media), and social scientists who study the effects of certain forms of communication on people’s identities and groups’ identities. In the new project, we want to explore exactly what you suggest in your question, the idea that stories have multiple functions (they inform, entertain, challenge, motivate, persuade) and have different success conditions relative to those functions: an inaccurate historical report can be at the same time misleading, entertaining, and motivating. I think an analysis of the role of stories is timely and urgently needed in the current political climate, where stories are used as arguments and have proven to be very powerful at influencing people’s thoughts and actions.
Does your project connect with thinking about metaphor and illness? The benefits, or potentially harmful effect, of common cultural metaphors as ways of visualising illness and recovery?
Not specifically. In the delusion and confabulation literature the notions of metaphor and metaphorical meaning have been explored to some extent, especially among those scholars who claim that we should view delusions and confabulations not (just) as beliefs, but as fictional expressions of thoughts and feelings or as descriptions of an alternative reality that the person recognises (at some level) as non-actual. I believe this may be an interesting approach to some cases of delusion and confabulation, but for independent reasons I prefer to view most delusional reports and confabulatory explanations as expressions of a literal truth that the person is committed to.
Illness as Fiction examines factitious illness narratives: people constructing elaborate fabrications about having a serious illness that they don’t really have. This is usually because they have an underlying psychological condition (such as Munchausen syndrome) and crave the attention and sympathy they receive as a result of the performance of the illness. Have you used any case studies of Munchausen syndrome / factitious disorder in your work? If so, how does this play out as a delusional belief or distorted truth: what are the redeeming features?
We have not addressed Munchausen syndrome as such. Rather, some of the delusion and confabulation literature focuses on a very interesting phenomenon that is probably the mirror image of Munchausen syndrome, anosognosia. ‘Anosognosia’ comes from the Ancient Greek and means literally ‘denial of illness’. It occurs when people acquire a severe impairment but fail to acknowledge either the impairment itself or the impact of such impairment on their lives. Most of the studies I have seen concern anosognosia for the paralysis of a limb. So, people who have become paralysed as a result of an accident, for instance, may deny that they have a mobility issue. They are often ready to justify their denial in the face of challenges from third parties. When asked why they do not climb stairs, they do not say: “Because I am paralysed” (which would be the truth) but “Because I have arthritis” (which is a confabulation).
Whether and to what extent anosognosia has some benefits to the person experiencing it, is controversial. Some have observed that when the person does not admit to being impaired, it is difficult for her to engage in rehabilitation or otherwise cooperate with her clinical team, resulting in poorer outcomes, as well as in tensions with her family and friends, due to the clash between her version of reality and theirs. However, some other studies have found that among people with the same impairment, those who have anosognosia report higher levels of wellbeing and lower levels of anxiety, probably because anosognosia has a protective function, shielding the person from the strong negative emotions that would ensue from the truth of her new severe impairment and the dramatic change in her future prospects. It is possible that anosognosia has some temporary psychological benefits, then, enabling the person to adapt gradually to the reality of her new condition and to keep depression at bay.
I was recently interviewed by Professor Lisa Bortolotti for her research blog Imperfect Cognitions: Lisa leads a research team working on delusional beliefs, distorted memories, confabulatory explanations, unrealistically optimistic predictions, and implicit biases — all topics that potentially overlap with fake illness narratives. You can read my interview here: I found the questions very inspiring, especially the (difficult!) one on the possible benefits of false accounts of illness. What do you think?
The second workshop of the Illness as Fiction project, led by Dr Maria Vaccarella, took place at the University of Bristol on Thursday 20/9/18, and focused on fictional and autobiographical cancer stories. As my research considers representations of women’s bodies as divine, and the ‘pathologizing’ of female sexuality, I am a loyal attendee of Maria’s workshops. I am particularly interested in the idea that fake illness narratives often employ a narrative of salvation, or ‘saintly’ cures; a trope we often encountered in the first workshop. We started the day’s session with an ice-breaker which was, quite aptly, somewhat religiously-themed: with the help of Post-it notes, we anonymously ‘confessed’ whether we had faked an illness to get out of social commitments. The ‘confession board’ looked like this:

After rejoicing that I wasn’t the only one who had lied about period pains, I wondered what separates such utterances from ‘malignant’ fabrications of illness narratives.
Maria, then, started by briefly introducing the project and the previous workshop, and by updating us on the progress of the project so far. She opened the day’s discussion with the provocative notion that fake illness narratives may be the purest form of illness narratives, as they present an illness which has no reality outside the text. Quoting the foundational essay by Susan Sontag, ‘Illness as Metaphor’, Maria reflected on the use of ‘prominent’ illnesses (such as cancer) as metaphors in cultural conversation, an ultimately damaging phenomenon for the people actually suffering from the illness, which alerts us to the difficulties involved in narrativizing illness.
During the morning session we had three presentations on different iterations of fake illness narratives. The first speaker was Louise Benson James, doctoral student in the Department of English at Bristol and Research Assistant for Illness as Fiction, who told us about her work to build a database of fake illness narratives. Ranging from literary to internet-based examples, her database is an effective way to find patterns in the illness narrative genre. Her database is divided into four categories: print texts, scholarship, Munchausen by Internet and online deceptions. Rather than trying to perform her own ‘hoax-hunting’, when it comes to internet sources, she decided to list only internet hoaxes that had already been disproved. Online hoaxes pose specific challenges, as the pages are often taken down once the creator is found to be lying. Louise’s project is ongoing, so more categories might emerge as the research progresses, and more texts will be added to the list!
Second on the lineup was Dr Sophie Stammers, Research Fellow at the University of Birmingham where she works as part of the PERFECT Project. This project, whose name is an acronym for Pragmatic and Epistemic Role of Factually Erroneous Cognitions and Thoughts, wants to establish the potential benefit to people’s social and/or mental wellbeing of beliefs that are false or irrational. Sophie spoke to us specifically about her work on confabulations, i.e. a story or explanation which is false but has no malicious intent, as it is based on a false memory or belief. Sophie interestingly connects confabulations with Fisher’s concept of ‘resonance’: the ‘confabulated’ explanation is such because it ‘strikes a chord’ with the speaker or their audience. Sophie raised interesting questions on the extent to which these kinds of confabulation have a positive effect on someone’s wellbeing and their social life, and what role they have in someone’s recovery narrative.
Last but not least, Dr Jurek Kirakowski (Cork) presented his work with Dr Aideen Lawlor on Munchausen by Internet (MBIs, feigning illness online) as displayed in Online Support Groups (OSGs). While OSGs are constructed to provide people suffering from a disease with empowerment, connection and support, they are also fragile, as they do not provide ‘tangible’ connections, and they are also fertile ground for MBIs. Jurek explained that MBIs display some of the psychological characteristics of the con artist, such as misinforming and causing hopelessness, in order to feed an emotional need. These practices have negative effects on real sufferers: some will edit their real accounts to conform more closely with the fake MBI’s account, and all users feel manipulated. One particular difficulty in detecting MBIs is that, once they are suspected of lying, they usually get expunged from online forums. Despite the many difficulties, one key characteristic Jurek identified is that they tend to define themselves by their illness, whereas genuine users usually want to move ‘beyond’ their condition.
The presentations sparked a lively discussion between the audience and the speakers, ranging from distinctions between a pathology of delusion and everyday instances of lying as social functioning, to the different paths of recovery in cases of confabulation and MBIs. These discussions in turn moved us smoothly to the more hands-on activities of the afternoon session. First, we tested the boundaries between fact and fiction by trying to guess whether a text was a novel or a memoir from reading selected passages. As someone who scored an embarrassing 3/10, I can testify that the boundary is more slippery than it might seem!
After this exercise, we considered ‘the clichés that cause the trouble’, in the words of Jeanette Winterson in Written on the Body, here with reference to the frequent use of clichés and specific metaphors in cancer narratives. Starting from a chart of cliché language and illness compiled by Jack Coulehan (‘paternal metaphors, ‘war metaphors’ and ‘engineering metaphors’), we moved to our next and final activity. Splitting into two groups, we joined forces for a collaborative textual analysis of two different excerpts from cancer narratives, The Fault in Our Stars by John Green, and ‘The Poetry Fox (and Other Tales from the Cancer Center’ by Nina Riggs – the former a novel, and the latter a memoir in blog form. We were tasked specifically with looking for the use of cliché language related to cancer, and whether there were attempts to overcome such language. These extracts led us to discussions about the nature of ‘telling’ illness, the possibility of subverting those clichés, and whether patients can really choose how to express their illness or feel like they have to conform to a specific vocabulary for their symptoms to be recognized and believed. A conclusion which leaves many interesting questions open for discussion at the next workshop!
Head over to The Polyphony to read my reflection on Workshopping the Medical Humanities – my call for slow-paced, less packed, but more engaging academic meetings. The first workshop for Illness as Fiction gets a mention, too. Thanks to Katrina for facilitating all this!
 Quinn Dombrowski,
Quinn Dombrowski,I’m delighted to announce that registration is now open for our second workshop “Malignant Fictions”.
For the morning session, we will be joined by two guest speakers: Sophie Stammers (Birmingham), who will present on confabulations, and Jurek Kirakowski (Cork), who will tell us about factitious disorder online. The collaborative textual analysis session in the afternoon will be devoted to cancer narratives this time.
Join us if you are interested in factitious illness memoirs, autofiction or, more in general, in the overlap between psychology and literature!
Attendance is free and lunch will be provided, but places are limited, so please book here.
Looking forward to seeing you in Bristol on 20th September!
On arrival at the first of a series of workshops for Dr Maria Vaccarella’s new research project on fictitious illness narratives, we were encouraged to share our reasons for attending. As someone who works on anxiety in contemporary American literature, I’m always fascinated to hear people’s thoughts on the slippery boundary lines between fiction and non-fiction – an interest shared by many researchers at the workshop. Others were keen to hone their skills of textual analysis in the context of the medical humanities, and to explore the narrativisation of symptoms, the relationship between psychoanalysis and the literary field, and how the day’s themes might map on to visual fictions.
The morning began with a paper from Professor Sue Vice on Tristan Szente’s self-published illness memoir Becoming Me (…Again) (2016), which details the aftermath of a motorbike accident, and subsequently, a mysterious brain virus. Sue considered how texts such as this often only truly come into being once their falsity is exposed, and how symptoms are used almost as excuses to account for discrepancies and contradictions in-text. She raised some particularly interesting questions about the gendered response to illness narratives, and how memoirs written by women are more likely to be questioned and distrusted, while also examining our motives for interest in narratives of illness and victimhood, which offer an existential appeal through tales of miraculous recovery and saintly cures. She concluded with thoughts that recurred throughout the day on the distinction between accounts of illness that are posted online and those that are published, particularly in relation to how these different forms are received.
Next up was Katrina Longhurst, who presented on Lauren Slater’s Lying: A Metaphorical Memoir (2000), a puzzling text which is self-conscious about the reader’s expectations of truth, opening with the words “I exaggerate.” Katrina thought through how the text operates as a form of counter-diagnosis, with language subverting diagnostic urges and embracing the sense of confusion and disjointedness illness may cause. Indeed, she also reflected on how this is a book which shifts and distracts itself; its narrative is repeatedly caveated, and, in Katrina’s words, stretches the autobiographical pact to breaking point. In this sense, she argued that Slater invites us as readers to enter the confusion of diagnosis with her – to face the multiple truths and voices of mental illness communally. This paper raised fascinating questions about the author-reader (and narrator-reader) relationship in illness narratives, while also contemplating on our reliance on diagnosis as truth, and what, if anything, a ‘true’ or ‘accurate’ illness narrative looks like.
This was followed by a paper from Dr. Maria Vaccarella, who provided an overview of her project and the questions that prompted it: what counts as an illness narrative today? Are they always artistic or performative, and if not, what else might they be? And why do we like them? In particular, Maria’s work is examining false accounts of illness, asking what cultural work is being done by these accounts, and what drives them, beyond narcissism and a desire for fame. Celebrity patients such as Belle Gibson, who wrote a cookbook and developed an app detailing her cancer diagnosis and subsequent health journey, have contributed to Marc D. Feldman’s concept of Munchausen’s by Internet – lying about one’s health online. Maria also reflected on the difficulties this can cause while researching, as many accounts of illness that are posted online and proved to be false are subsequently deleted very promptly. One notable trend throughout the morning’s papers was that writers who created false illness narratives often drew very heavily on the work of their idols – Sue’s paper considered how James Frey’s A Million Little Pieces (2003) borrowed scenes and phrases from Charles Bukowski’s Ham on Rye (1982), and Maria noted how Gibson drew her approaches from a real cancer patient and wellness writer called Jessica Ainscough. This points to the implicit intertextuality of false illness narratives, which model themselves on the accounts of real patients, taking the reader along for the journey of emotions that follow when this falsity is exposed. Maria referred to the complex relationship between online accounts and health promotion as the new melodrama of social media autofictional storytelling, which is also at the heart of her new work.
These papers prompted a wide-ranging discussion on medical charlatans, models of miracle cures, reader responses to the exposure of illness narratives as fake, ethical questions as to when crime begins in the creation of false illness narratives, and, perhaps most interestingly, the remedicalisation of such texts, where they are recuperated as symptomatic of real conditions such as factitious disorder. In turn, this moved us into a brilliant Fact or Fiction exercise, where we were asked to identify whether passages of writing were fictional or non-fictional (at least when initially marketed!). In doing so, we were able to further discuss our expectations of accounts of illness – are there clear markers of falsity in-text? How might language and narration differ when comparing fictional and non-fictional accounts of illness? This was followed by a ‘new title’ activity, where we were asked to think about whether, and how, we would rename autobiographical texts that are revealed to be false, which again raised questions of how readers react to discovering a text is not what it seems.
To close the day, we came together in groups to analyse extracts from fictional and non-fictional accounts of illness, including some non-fictional writing that was revealed to be false. Drawing on Anne Hawkins’s Reconstructing Illness and Arthur Frank’s The Wounded Storyteller, we reflected on some common genres or narrative trajectories within illness narratives, from the idea of rebirth (illness as an occasion for spiritual growth) to quest and chaos narratives, which respectively frame illness as a journey of discovery, and as anti-narrative, with bodily confusion reflected in a text’s plot. During these discussions, I was interested by the way in which we as readers tend to introduce personal anecdotes into our analysis of illness narratives – it’s as though we feel some compulsion to relate these stories to our own experiences, deepening both the author-reader relationship, and the sense of deception when their stories are revealed to be fake – all food for thought for our next session!